Told No to Dental Implants? Why a Specialist Second Opinion Often Says Yes
Medically reviewed by Dr. Alexander V. Antipov, DDS — Board-Certified Oral & Maxillofacial Surgeon · Diplomate, American Board of Oral & Maxillofacial Surgery (ABOMS) · California Dental License #50724
What if the "no" you received wasn't a final verdict, but simply a limitation of the tools used to reach it? Being told you lack the jawbone for a permanent smile is discouraging — especially when you are already dealing with shifting dentures or a visible gap. But the reality of implant eligibility has changed dramatically. Studies report clinical success rates near 98% even for implants placed in grafted bone, and modern 3D imaging routinely finds usable bone that flat X-rays miss entirely. This guide explains why bone recession is a hurdle rather than a finish line, why a general practice's "no" so often becomes a specialist's "yes," and why waiting is the one choice that genuinely works against you.
TL;DR
- • "Not enough bone" is usually a statement about what standard tools can see and do — not a permanent diagnosis of your jaw.
- • Traditional 2D X-rays show bone height but hide its width; 3D CBCT scans routinely reveal hidden bone volume that makes implants possible.
- • Bone loss is progressive, and conventional dentures accelerate it — waiting for the "perfect time" only shrinks your options.
- • Modern techniques — grafting, angled placement, and full-arch protocols — turn most "impossible" cases into workable plans.
- • Eligibility depends on bone quality and strategic placement, not just quantity, which is why a surgical second opinion matters.
Why "Not Enough Bone" Is Rarely a Final Answer
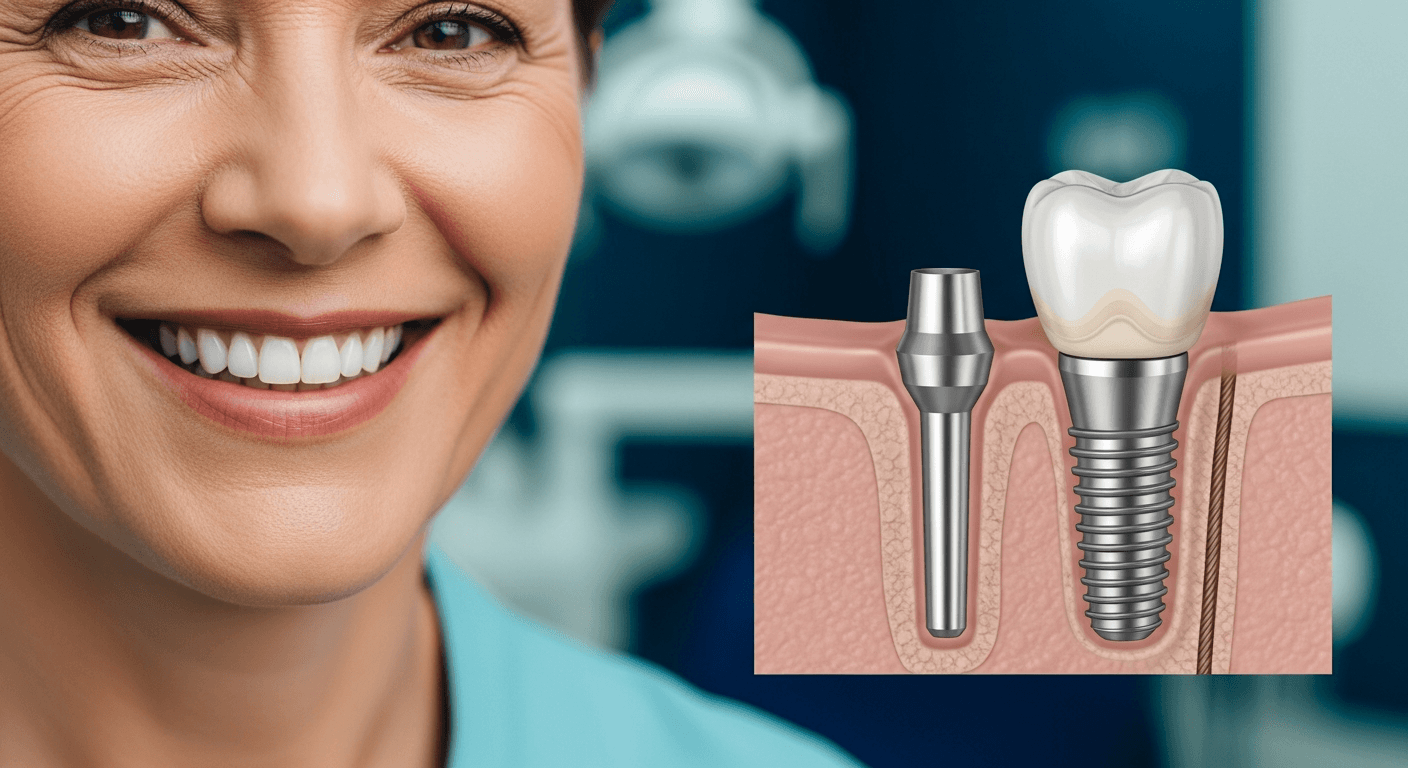
Many patients arrive discouraged after being told their jawbone is too thin for implants. The medical term for this thinning is resorption: bone needs the constant stimulation of a tooth root to maintain its density, and when a tooth is lost, the body begins recycling that bone elsewhere. Years of missing teeth — or of periodontal disease actively eroding the foundation — can leave a jaw that looks, on a standard exam, like it has nothing to work with.
But the myth that "not enough bone" is a permanent disqualifier is outdated. Early implant dentistry required a large volume of natural bone for traditional placement. Modern surgical planning uses the bone you still have far more efficiently — anchoring in the densest available areas, angling implants to engage more bone, and rebuilding volume where it is genuinely needed. Today, the deciding factor is no longer just how much bone remains, but its quality and where it sits.
2D X-Rays vs. 3D CBCT: Why the Same Jaw Gets Two Different Answers
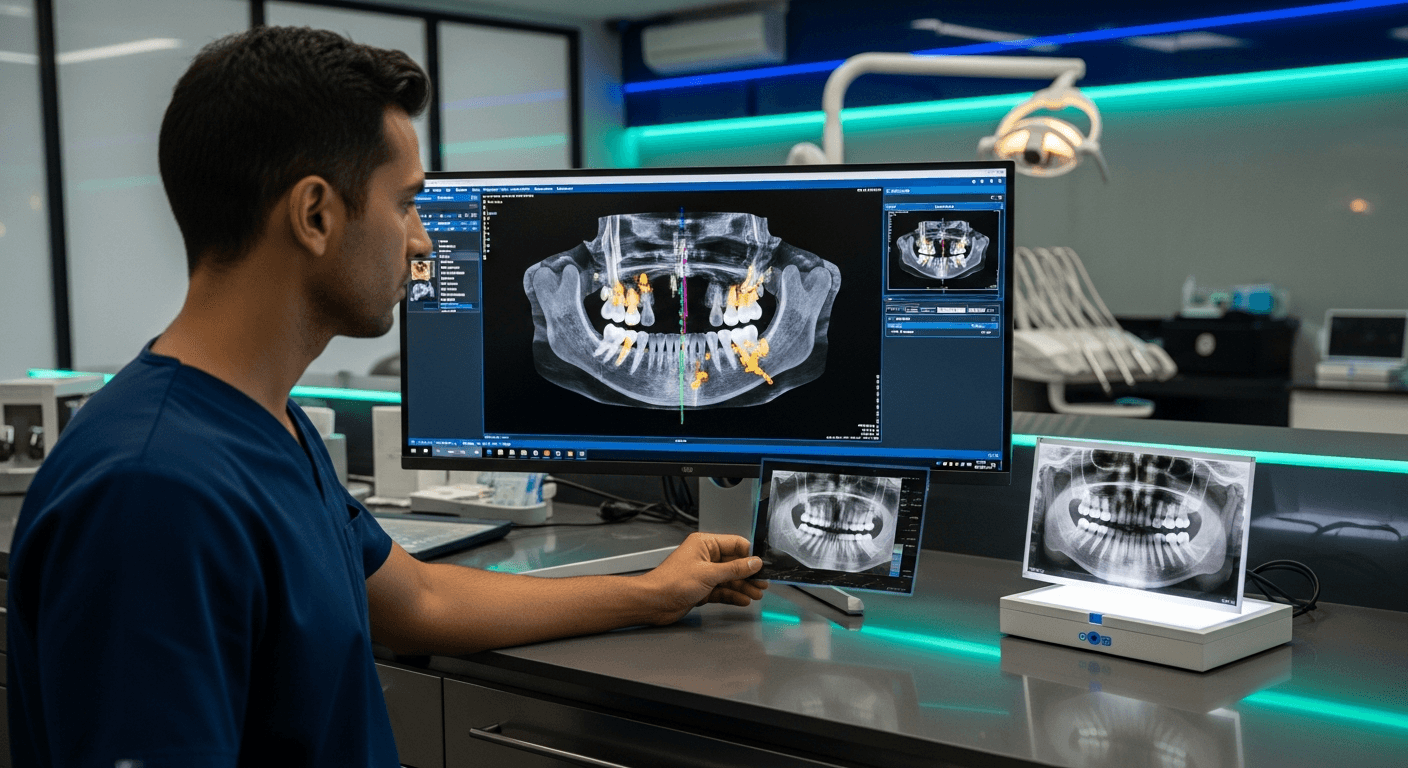
Here is the most common reason a general dentist says no while an oral surgeon says yes: they are literally looking at different pictures. Standard 2D X-rays are like looking at a shadow on a wall — they show the height of the bone but hide its thickness and density. A jaw can appear hopeless in a flat image while still containing usable "pockets" of dense bone invisible to that technology.
A cone-beam CT (CBCT) scan builds a three-dimensional digital map of your entire jaw with sub-millimeter precision, revealing the exact width, depth, and density of the bone — and the precise position of nerves and sinuses. That map is what allows a surgeon to find stable anchor points a 2D image simply cannot show. It is also the basis for guided placement: see how 3D planning improves implant accuracy.
The difference in training matters too. A board-certified oral and maxillofacial surgeon completes years of hospital-based surgical residency focused on jaw anatomy, bone grafting, and anesthesia — the exact skill set complex, low-bone cases demand. A practice without that equipment and experience isn't wrong to say no; it is saying no to what that practice can safely do.
The "Waiting Game" Trap
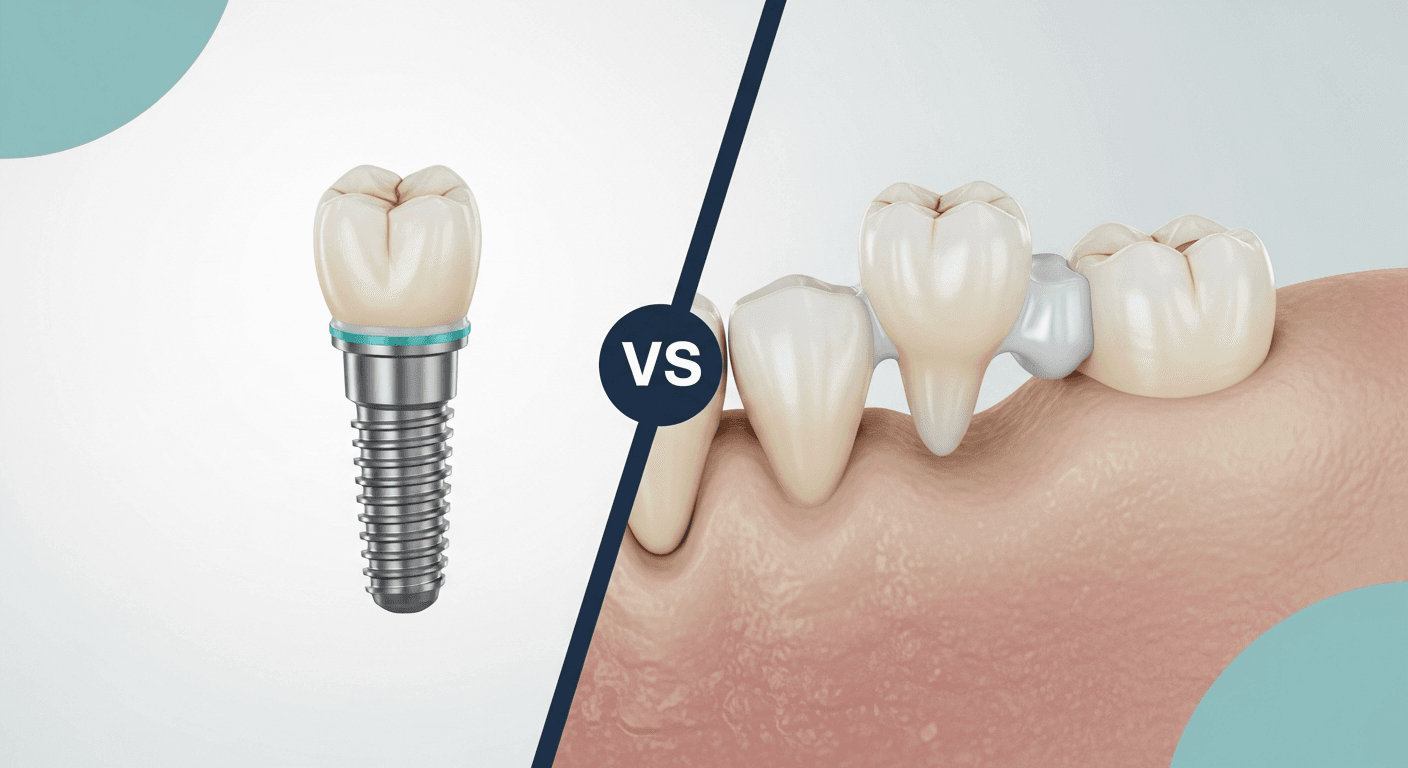
Waiting for the perfect time to act is one of the most costly mistakes in implant dentistry, because bone loss is progressive — it does not stop on its own. Conventional dentures often make it worse: they sit on top of the gums and apply uneven pressure that accelerates the thinning underneath, which is why dentures fit worse every year. It is a self-reinforcing cycle — the longer you wait, the less bone remains and the more involved the eventual fix becomes. For the full comparison of how the two paths diverge over time, see implants vs. dentures.
The practical takeaway: a specialist evaluation sooner rather than later doesn't commit you to surgery — it stops the clock on uncertainty. Knowing exactly how much bone you have, and how fast the situation is changing, is what lets you choose your timing instead of having it chosen for you.
How Specialists Turn a "No" Into a Plan
Once a 3D scan maps the real anatomy, most "impossible" cases resolve into one of a few well-proven strategies. Where volume is genuinely missing, grafting rebuilds it — from minor socket preservation to sinus lifts in the upper jaw. Where grafting can be avoided, angled or shorter implants engage the dense bone that remains. And for a failing full arch, protocols like All-on-4 tilt the rear implants specifically to work around resorbed areas. The complete menu of options is covered in our guide to dental implants with severe bone loss.
The important point for a patient who has been turned away is that these aren't experimental workarounds — they are standard-of-care techniques in surgical practices, with success rates comparable to implants placed in native bone. What varies is not the biology; it is whether the practice you consulted has the imaging, training, and case volume to offer them.
What a Complex-Case Consultation Actually Looks Like
A meaningful second opinion is more than a quick look at the gap in your smile. At a surgical consultation, the evaluation starts with a CBCT scan and a review of your full medical history — healing capacity, medications that affect bone (such as bisphosphonates), smoking status, gum health, and prior dental work. The goal is to assess the biological potential of your jaw, not just its current limitations.
From there, planning happens digitally: the surgeon places your implants on a 3D model of your jaw first, locating the densest anchor points before any incision is made. That precision typically means shorter surgical time, less tissue trauma, and a more predictable recovery. It also produces an honest, itemized answer about what your case requires — and what it doesn't. Learn what to expect at your first visit on our consultation page.
A Second Opinion With Dr. Antipov in Roseville
If you have been told you aren't a candidate for implants, that conclusion deserves to be tested against a 3D scan and a surgeon's eyes. Dr. Antipov is a board-certified oral and maxillofacial surgeon in Roseville who focuses on exactly these complex and previously declined cases — from single sites with thin bone to full-arch restorations after years of denture wear. Most implant "failures," and most premature "no's," trace back to planning and bone support, not to a patient's body rejecting treatment; a careful surgical plan changes both. If your concern is an implant that was already placed and is now struggling, see our guide on getting a second opinion on failed dental implants.
Frequently Asked Questions
My dentist said I don't have enough bone for implants. Is that final?
Usually not. That assessment is often based on 2D X-rays, which show bone height but hide its width and density. A 3D CBCT scan frequently reveals usable bone that flat images miss, and surgical techniques like grafting and angled placement can work with — or rebuild — what remains. A specialist second opinion is the only way to know for sure.
Why would an oral surgeon say yes when a general dentist said no?
Two reasons: imaging and training. Surgical practices use 3D CBCT scans that map bone in three dimensions, and board-certified oral surgeons complete years of hospital-based residency in jaw anatomy, grafting, and anesthesia. Both allow them to safely treat low-bone cases that fall outside what a general practice is equipped to handle.
Does waiting to get implants make bone loss worse?
Yes. Bone loss is progressive and does not stop on its own — and conventional dentures accelerate it by pressing unevenly on the gums. The longer a jaw goes without root stimulation, the more bone resorbs and the more involved the eventual treatment becomes. An early evaluation preserves your options even if you choose to treat later.
Can my body reject a dental implant?
True rejection of medical-grade titanium is extremely rare. Most implant failures trace back to inadequate planning, insufficient bone support, or infection — all of which are addressed by careful 3D planning and site preparation. That is why implants placed even in grafted bone report success rates near 98%.
Will I definitely need bone grafting if I've had bone loss?
Not necessarily. 3D planning often finds enough dense bone to place implants without grafting, using angled or strategically positioned implants. When grafting is needed, it ranges from a minor same-day addition to a staged sinus lift. The scan determines which path applies to your anatomy.
What should I bring to a second-opinion consultation?
Bring any prior X-rays or scans, a list of medications, and notes on what you were told previously. The consultation will add a 3D CBCT scan and a full surgical assessment, then give you a clear, itemized answer about your candidacy and the specific plan your jaw supports.
Get a Second Opinion Before You Accept "No"
If you've been told you can't have dental implants, let a board-certified oral surgeon look at your case with 3D imaging. Dr. Antipov evaluates complex and previously declined cases at his Roseville office — schedule a consultation to find out what your jaw actually supports.
Book a Free Consultation