Severe Overbite: When Jaw Surgery Is Needed
Medically reviewed by Dr. Alexander V. Antipov, DDS— Board-Certified Oral & Maxillofacial Surgeon · Diplomate, American Board of Oral & Maxillofacial Surgery (ABOMS) · California Dental License #50724
Most overbites can be fixed with braces or aligners, but severe skeletal overbites — where the jaw bones themselves are misaligned — need jaw surgery, known as orthognathic surgery, explains Dr. Alexander Antipov, a board-certified oral & maxillofacial surgeon in Roseville, CA. Here is how to know which applies to you.
This article is for general education — consult a qualified oral surgeon or orthodontist for a recommendation tailored to your case.
When Is Jaw Surgery the Right Answer?
Most overbites can be corrected with orthodontics alone. Jaw surgery (orthognathic surgery) becomes the right answer when:
- — The overbite is skeletal in origin (the jaw bones are misaligned, not just the teeth).
- — The overbite is severe (typically 9+ mm overlap).
- — Functional problems are present — chewing, breathing, sleep apnea, TMJ pain.
- — Previous orthodontic treatment failed or relapsed.
- — The facial profile is significantly affected.
- — The patient wants a stable, permanent correction.
For these cases, orthodontics alone produces limited or unstable results. Surgery addresses the underlying bone positioning.
What Is Orthognathic Surgery?
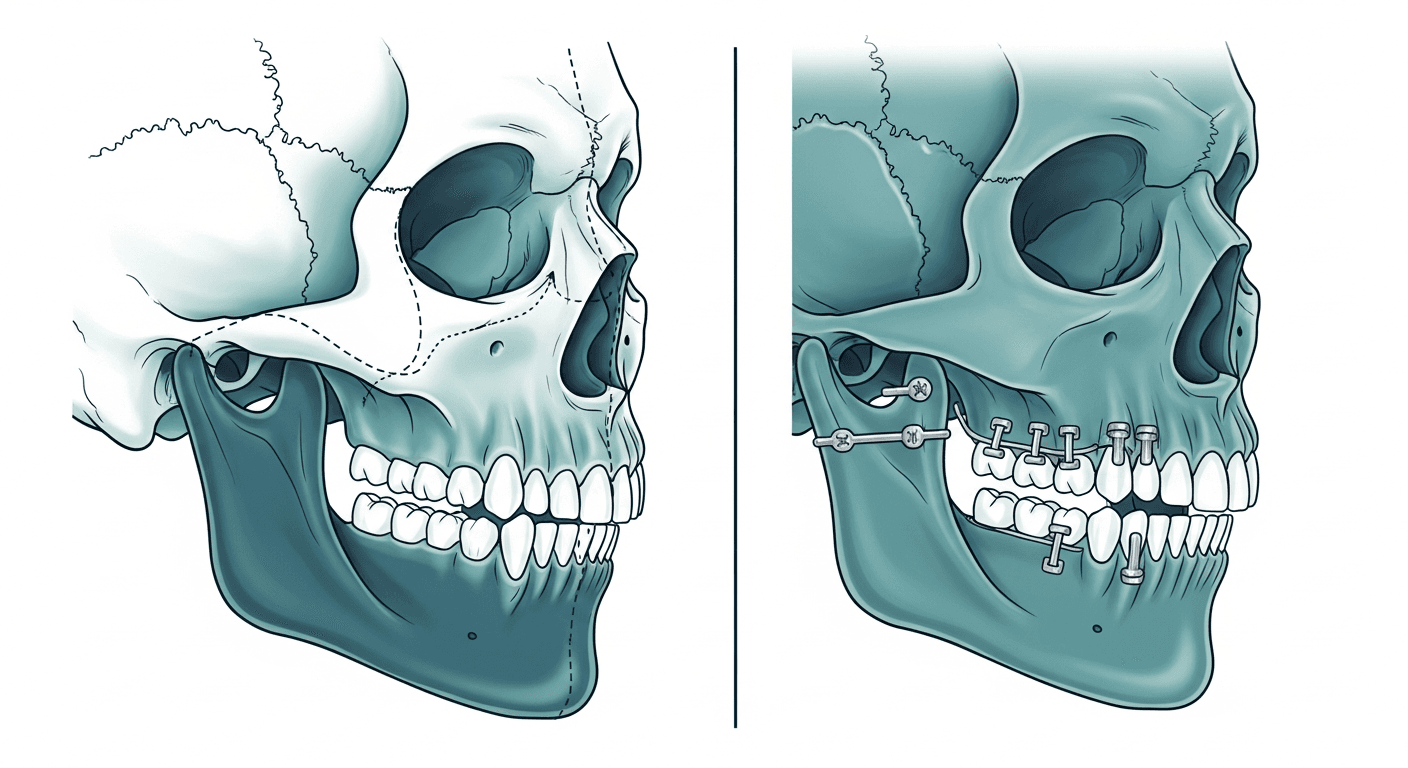
Orthognathic surgery repositions the upper jaw (maxilla), lower jaw (mandible), or both. The bones are surgically separated, moved into proper position, and secured with small titanium plates and screws. For overbite correction, the most common procedures are:
- — Maxillary impaction or setback (Le Fort I osteotomy). Used when the upper jaw is positioned too far forward or downward. The maxilla is repositioned to a proper position relative to the lower face.
- — Mandibular advancement (BSSO — bilateral sagittal split osteotomy).Used when the lower jaw is too far back. The mandible is moved forward to create proper bite alignment and improve facial profile.
- — Bimaxillary surgery. Combines upper and lower jaw repositioning for severe cases or maximum aesthetic improvement.
- — Genioplasty. Chin reshaping that may be combined with jaw surgery for facial harmony.
How Severe Is “Severe”?
Categories of overbite severity:
| Severity | Overlap | Typical Treatment |
|---|---|---|
| Normal | 1–3 mm | None needed |
| Mild | 4–6 mm | Clear aligners or braces |
| Moderate | 6–9 mm | Braces, sometimes with extractions |
| Severe | 9+ mm | Surgery often needed |
| Deep bite (gum impingement) | Upper teeth touch lower gum | Surgery typically needed |
Severity alone does not determine surgery. The cause (dental vs. skeletal) matters more.
Signs Surgery Might Be Right for You
You are more likely to be a surgical candidate if you have:
- — A significantly recessed chin or weak lower-jaw appearance.
- — A protruding upper jaw that cannot be camouflaged with orthodontics.
- — Persistent TMJ pain related to bite mechanics.
- — Sleep apnea with structural causes (maxillomandibular advancement is a treatment for severe sleep apnea).
- — Difficulty closing your lips at rest.
- — Speech difficulties related to jaw position.
- — Excessive gum show when smiling (a gummy smile from a skeletal cause).
- — An asymmetric face related to jaw misalignment.
- — Failed prior orthodontic treatment that relapsed.
A consultation with both an orthodontist and an oral/maxillofacial surgeon provides the clearest evaluation.
The Treatment Sequence
Orthognathic surgery is rarely “just surgery” — it is a coordinated 1–3 year plan with three phases:
- Pre-surgical orthodontics (6–18 months).Braces or aligners move teeth into the position they will need to be in after surgery — not the position they should be in given current jaw alignment. This can temporarily make the bite look worse.
- Surgery.Performed under general anesthesia, typically requiring an overnight hospital stay. Single-jaw surgery takes 2–3 hours; double-jaw surgery takes 4–6 hours. The bones are repositioned and secured with rigid fixation (small plates and screws). Recovery begins immediately.
- Post-surgical orthodontics (6–12 months). Final tooth movement to optimize the new bite. Retainers are then worn long-term.
Total timeline:typically 18–36 months from start to finish.
What to Expect from Surgery
Day of surgery: general anesthesia is administered through an IV. Surgery is performed entirely from inside the mouth (no facial scars), the bones are repositioned and secured with hidden hardware, an overnight hospital stay is typical, and significant facial swelling is expected.
First week:substantial swelling peaks at days 3–5, a liquid diet is required, pain is managed with prescribed medications, and jaw movement is limited. Most patients miss 1–2 weeks of work or school.
Weeks 2–6: swelling gradually subsides, a soft-food diet is introduced, and patients return to light activities. Numbness in the lips, cheeks, or chin is common and usually resolves over months.
Months 2–6: bone healing continues, patients return to all activities, final orthodontic adjustments begin, and sensation gradually returns.
Long term:bone fully heals over 6–12 months, the hardware (plates and screws) typically remains in place permanently, and retainers are worn for life.
Risks and Realistic Expectations
Orthognathic surgery is major surgery. Realistic risks include:
- — Numbness in the lips, cheeks, or chin — common; usually improves over months but can persist.
- — Infection — rare with proper antibiotic prophylaxis.
- — Nerve injury — typically temporary; rarely permanent.
- — Bite changes from healing — sometimes require post-op orthodontic adjustment.
- — Need for revision surgery — rare but possible.
- — General anesthesia risks — standard for major surgery.
- — Hardware-related issues — rare; sometimes requiring removal years later.
The majority of properly evaluated and prepared patients have excellent outcomes with significant functional and aesthetic improvement.
Cost and Insurance
Total cost typically breaks down as follows: the surgery itself runs $20,000–$45,000, orthodontics (before and after) add $5,000–$10,000, and hospital and anesthesia costs are included or additional depending on the setting. The complete plan generally falls in the $25,000–$60,000 range.
Orthognathic surgery is often covered by medical insurance(not dental) when documented functional impairment exists (chewing, breathing, sleep apnea), conservative treatment has failed, and specific medical-necessity criteria are met. Many patients have 60–90% of surgery costs covered by medical insurance, with orthodontics covered partially by dental insurance.
Why Choose Surgery Over Camouflage?
For skeletal overbites, surgery has clear advantages over orthodontic camouflage:
- — Stable, predictable results that do not relapse.
- — Functional improvements — chewing, breathing, sleep.
- — Significant facial profile improvement when desired.
- — Treatment of associated conditions like sleep apnea.
- — Once-and-done rather than lifelong management.
Orthodontic camouflage in skeletal cases often produces compromised results, relapses over years, worsens TMJ symptoms, does not address the underlying problem, and may still require surgery later. For the right patient, surgery is the most efficient long-term solution.
When Surgery Isn’t Right
Surgery is not appropriate for:
- — Mild to moderate overbites that respond to orthodontics.
- — Patients with significant medical contraindications to general anesthesia.
- — Patients unwilling to commit to the timeline.
- — Patients who have not tried orthodontic options first for borderline cases.
- — Anyone making the decision impulsively — this is major surgery.
Frequently Asked Questions
How painful is jaw surgery?
It is discomfort, not severe pain. Most patients describe it as significant swelling and numbness rather than acute pain. Pain medication manages discomfort effectively.
Will my face look completely different?
For severe skeletal cases, yes — significantly. Most patients report the change as positive and aligning with how they always wanted to look. Subtle to moderate changes are also common.
How long until I look “normal” after surgery?
Major swelling resolves in 2–4 weeks. Substantial improvement is seen by 6–8 weeks. The final result is visible at 6–12 months.
Can I eat solid food after surgery?
Liquid only for the first 1–2 weeks, then soft foods through week 6. A full diet is typically resumed by 8–12 weeks.
Will the hardware set off airport metal detectors?
Modern titanium plates rarely trigger detectors. Carrying a surgical card may help if you are questioned.
Can I have jaw surgery if I’m older?
Yes. Adults of any age with adequate health are candidates. Bone heals well at any age.
Will I need braces forever afterward?
You will need retainers for life in some form, but braces themselves are typically removed 6–12 months after surgery.
Sources & References
Peer-reviewed and authoritative references supporting the information in this article.
Dr. Alexander V. Antipov
Board-certified oral and maxillofacial surgeon specializing in dental implants, full-arch restoration, zygomatic implants, and corrective jaw surgery. Serving patients throughout Northern California and beyond.
Wondering If Jaw Surgery Is Right for Your Overbite?
Schedule a consultation with our oral and maxillofacial surgeons. We will evaluate your case and explain every realistic option, including non-surgical alternatives. A patient coordinator will follow up within 24 hours.